
It’s always good when traveling to keep an eye out for opportunities to explore something off the usual tourist trail and this trip I found out how things work inside a Thai hospital. All the staff, medical and administrative, wear the most stylish uniforms and do everything with utmost professionalism. My key contact there told me he had been trained for 6 years in Sydney, Australia. But slightly veering off the usual day-to-day experiences opens one’s eyes to little things where values and expectations differ in sublte ways from what we expect in Australia and probably many other white English speaking countries.
For one, when my contact (who is responsible for international visitors to the hospital) introduced the nurse who would be the one responsible for my immediate care he introduced her with “This most beautiful lady’s name is ….” Things like that immediately hit one in a way to remind us Westerners at least that we have a whole different social thing going on with feminism and how men have to learn to do things differently from the way they were done in the old days. At least where I worked — in public universities and libraries — such a manner of addressing a woman in a professional situation would always be considered inappropriate. (He spent 6 years in Sydney but the Thai customs never left him.)
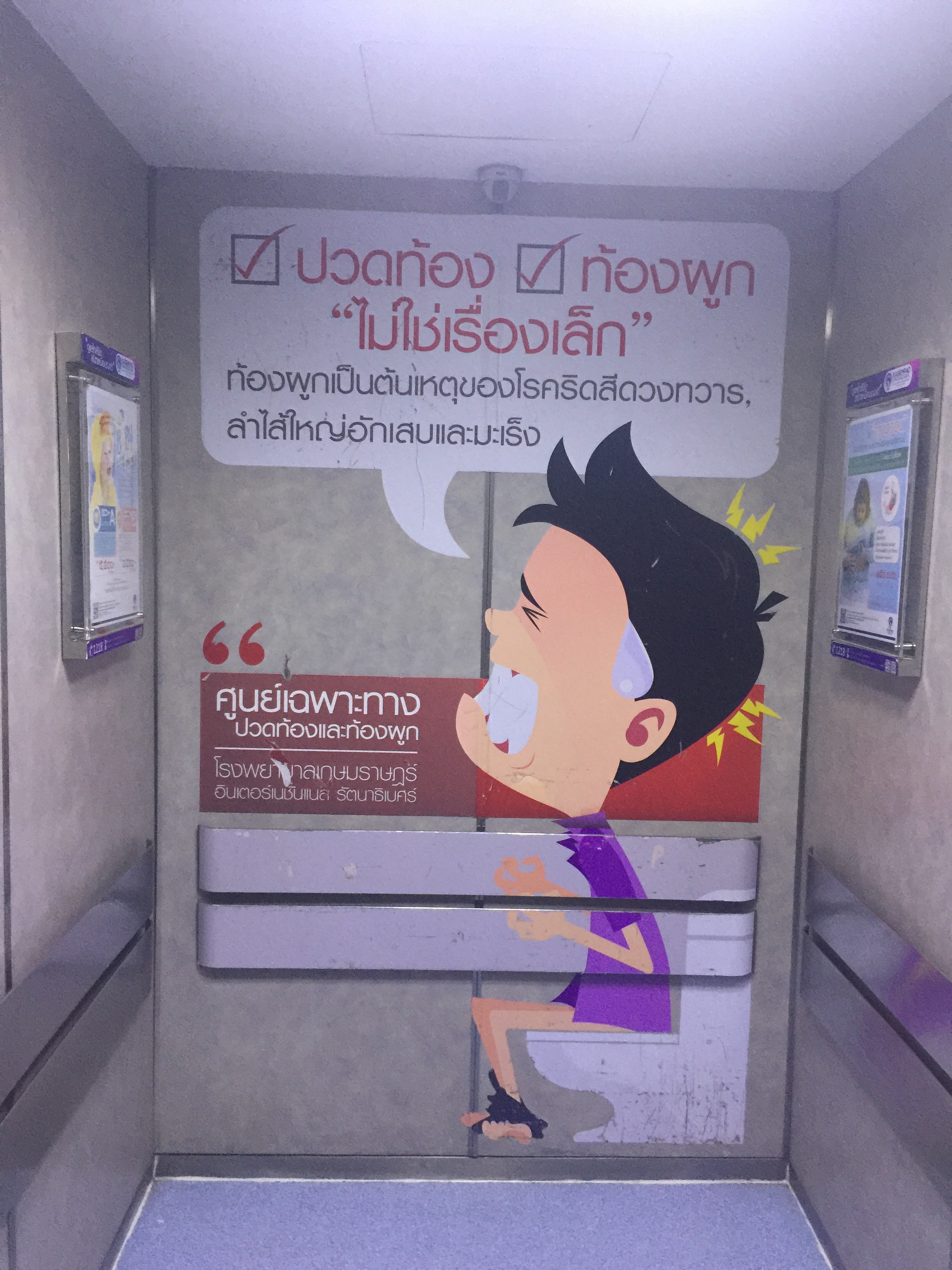
Then there was this. The day I was discharged I was being wheeled out and for the first time I saw the walls around me and not just the ceilings …. now I don’t know about other Anglo-Saxon countries, but I have a feeling that we would be most unlikely to be confronted with the following cartoon figure in such a place, (or is my experience of hospital murals way too limited?)
Actually before I went to the hospital I was looking for an ordinary doctor somewhere and following helpful directions I came to an area where there were sort of nurse-like-uniformed girls standing outside a shop handing out flyers, presumably to encourage people to enter — I wasn’t sure if it was actually a doctor’s surgery so I looked in and asked the woman I thought was the receptionist at the front desk for a doctor and she replied that she was the doctor and asked how she could help. There was a quick diagnosis over the counter …. But I will not want to leave the impression that that’s how all doctors here operate! Nor would she always service all clients that way.
Anyway, it was all a very interesting experience, something different, which I always look forward to. Oh, one more detail. When being discharged I was handed a form to fill out. It consisted of dozens or questions — but all in Thai — which I learned were asking me how I felt about their service, would I ever like to use them again, would I recommend them to someone else, that sort of thing, I think. I scarcely know the Thai alphabet so I left it aside.
And while talking of different things, here are a couple more.
I was in an outlying “suburban” area of Bangkok (though it was more like a city centre in many places in Australia) and was waiting responsibly at the lights to cross the road. When they turned green to signal me across I stepped out but not a damn car or motor bike seemed to notice that they had a bloody red light! There must have been about a dozen cars and bikes that just kept on driving through and weaving their way around me. It was a stimulating experience, that’s for sure. Usually cars stop at red lights, even here. But obviously not always. And when I reached the other side I passed two police officers nonchalantly walking back to their vehicle with their purchased lunches.
Anyway, I went into a chemist and asked for something and they searched frantically everywhere for me but couldn’t find what I wanted, so with their smiling apologies I left. I must have been about 50 metres down the street when I heard a woman shouting. She reached me to show me that she had finally found what I was asking for. It wasn’t quite what I was wanting but I couldn’t disappoint her after making such an effort so I returned with her and made the 39 baht ($A2) purchase.
Beer is not such a big deal here. Every shop sells it and sometimes the staff helpfully add a straw before you take it away. I know you won’t believe me so I took a photo to prove it’s true.
If you enjoyed this post, please consider donating to Vridar. Thanks!
The funny thing about that mural is that the person looks Anglo, not Thai. Do you have any idea what it says?
Also, an irony about Western culture is that we get so much criticism regarding sexism and racism, but this is really only because we are the most progressive on these issues so that it’s even acceptable to discuss it. These issues aren’t even addressed in most other cultures because they are more racist and sexist.
It says that stomach ache and constipation or bleeding anus may not be minor things but could be symptoms of cancer or something like that.
(I don’t think anyone here would consider him particularly western in appearance.)
Possible translation:
[/] Abdominal pain
[/] Constipation
“Do not quit” [→possible social reference (type:humorous) ???]
The stomach is the cause of hemorrhoids, inflammation and cancer
Correction:
ไม่ใช่เรื่องเล็ก —not a small problem [rather than “Do not quit”]
the person looks Anglo, not Thai
It is probably a psychological feature like “Pareidolia”, that when viewing an image of a human with no exaggerated features (phenotype, culture, etc.), then the viewer will perceive the human as similar to themselves per phenotype, culture, etc.
Yeah, maybe so. Kind of a hard image to judge I guess.
Cartoon persons are very common here in public notices and advertisements and they are all obviously of Asian figures, so I was viewing this image in that context. In such images the hair is typical of youthful Asian, and black hair is ubiquitous among Asians, and here the eyes are squinted out. Maybe the pale skin here looks European but I can’t tell if that’s something to do with lighting of fading. Besides, skin colour among Asians, including Thais, varies a lot, from quite dark (mainly southern) to very light. (Some Asians appear whiter than the “typical us”.)
They do things differently here than here: medicine has become more than alien to me here in the US. I was not ever comfortable with US medicine personally, but it is now a different world, a different universe.
I worked for decades in US medical settings as well as having intermittently been a patient over decades. Long ago I worked briefly in settings in a 3d world country (albeit with a culture probably more like the US’s than Thailand’s is like Australia’s).
The differences in US medicine that have taken place in US medicine would take volumes to describe, but they include such overlapping trends as extreme moves towards overt commoditization, less time for history taking and physical examination, depersonalization, and increased regimentation in multiple respects. The technology of medicine itself has something to do with the change (many new tests and ways to analyze and display the tests!). However much has to do with the technology of billing, the efficiency of tracking apparent efficiency of medical care workers, the technology of record keeping, and so forth–also the introduction in the US of advertising in medicine, which was not many decades ago a taboo (“unprofessional”–you would never see doctors or hospitals advertise, for example). There’s the pushing of tasks onto patients to cut down costs, the increased inability of personnel to listen to each other or to patients because of their rush and need to multitask, medicine performed often by people with lesser training but using a carefully prepared script or computerized equivalent, very much with lawyers’ direct or indirect input. In many ways the medical setting of the very foreign country I knew decades ago might seem more familiar to me than the medical setting I experience now in the US.
Profit motive is clearly driving US medicine off the rails. I think a lot of the issues are driven by insurance companies and hospitals which are certainly run primarily from business perspectives. The biggest problem I think is that profit motive has totally undermined trust in our medical system to the point that people are reluctant to use medical services because we #1 don’t believe that medical professional have our best interest at heart, rather they are focused on maximizing profits, which means over-prescribing, over-diagnosing, not spending the time to make sure they get it right just it and see if ti works and bill for it, etc. and #2 because there is so much uncertainly with billing. Everyone knows now that any time you interact with the medical system in any way, you have no idea what is going to happen financially. You could walk away with no bill and everything is covered or a $100,000 bill that your insurer refuses to pay. It is literally impossible to have any idea what’s going to happen.
You can go in for some basic procedure in an in-network facility, its supposed to be covered and cost you only like $200 out of pocket, then once its all done you get hit with $50,000 bill because they called in an out-of-network anesthetists to come in and do like 20 minutes of work. Seriously this crap happens all the time.
It’s insane. Our medical “system” is complementary off the chain and out of control. It’s a disgrace.
There’s now relentless attention to cutting costs and increasing revenues–also concomitant attention to advertising about Caring and other gesturing towards sensitivity in interpersonal interactions.
It is not that many people in the system do not try. They are under tremendous stress. Often the ethical burdens are the worst of all. It is not for nothing that the alcoholism and suicide rates are high among physicians, that many retire early, and so forth. I do not know the stats so much with nurses, but believe it may be similar. Their stresses in some ways are less, in some ways far greater. Other medical workers as well experience the same stuff in different ways.
You put “system” in quotation marks. The word “Our” perhaps belongs in quotation marks.
(An irony: Between this note and the prior one above I received an electronic message from a prominent physician, probably one of the absolute best around, whom I am lucky to have, who indulges me. I think he answered me while on vacation. However I think he was so much in a hurry that he misread my original note. Not that what I wrote was necessarily any more clearly written than some of my notes here.)
A cynical follow-up note about some hospitals’ buyout offers to older nurses:
I have often wondered whether the offers of seemingly fairly generous cash offers for nurses who retire a little early might not just be for saving money. Could it be something along the lines of putting things–such as the nurses’ minds– down the memory hole? Do they want to delete remnants of the old culture? Perhaps they are deliberately disappearing nurses who might complain about dangerous workloads or too little time to get to know patients really well so as to comfort them, or who might remember how nurses rather than less well trained (and cheaper) personnel did certain things not too long ago, nurses who might better know the importance of intuition of sensing how a patient might be turning sour without firm data, and so forth. Such older nurses might be undesirable influences. I might well be wrong. I do not know. Maybe it’s just to save the salary money. ( I wonder whether older personnel are being disappeared in other areas, such as in high tech, for analogous reasons, and not just to save money, but that’s another matter.)
(((Incidentally, I neglected a piece of irony in the note above about the great physician who seemed to have just responded to me w/o having read understood my note to him. This is someone who I believe gives lectures in earnest about the very issues we have been discussing. Rather than being on vacation as I suggested, he may be taking time from his ormally overloaded schedule, which includes administrative fighting over such issues, to travel to give lectures on the very problems we discuss. The stress lines are at the higher levels, at least among the more conscientious, as well as the lower levels.)))
Just when I thought we had it reasonably .good health-care-wise in Australia this morning this news item appeared online: Why the Pharmacy Guild is the most powerful lobby group you’ve never heard of. It’s one of those things we take for granted and don’t notice till a someone points out the details and makes us think about what we take for granted. Surely medication is a right and therefore should be publicly owned and administered.